January 12, 2024
A Medical Provider Survey on the Impact of Restoring Passenger Rail Service
Improving Access to Specialty Medical Care: A Medical Provider Survey on the Impact of Restoring Passenger Rail Service in Central Washington
Transport to Medical Care Presentation
AAWA has provided technical assistance to this survey, which was initiated and conducted by the Washington Physicians for Social Responsibility and the Pacific Northwest University of Health Sciences.
PRINCIPAL INVESTIGATOR:
Anthony Stephas, DHSc, PA-C
509.249.7917
[email protected]
STUDENT CO-INVESTIGATOR:
Gleb Sych
727.459.5419
[email protected]
PARTNERING ORGANIZATIONS & TECHNICAL ADVISORS:
All Aboard Washington
Charles Hamilton, PhD
Co-Executive Director
[email protected]
Gary Wirt
Vice-President
[email protected]
Washington Physicians for Social Responsibility
Breck Lebegue, MD MPH
[email protected]
DATE: January 12th, 2024
CONTENTS
1.0 INTRODUCTION
2.0 BACKGROUND
2.1 Primary Outcome Measures
2.2 Secondary Outcome Measures
2.3 Hypotheses
3.0 RESULTS
3.1 Specialty Care Cities
3.2 Respondents’ practice locations
3.3 Primary mode of transportation to specialty appointments.
3.4 Minimum train service required to benefit non-urgent patient transportation.
3.5 Respondent prior experiences with passenger rail
3.6 Extended Responses
4.0 ANALYSIS & DISCUSSION
4.1 Study Limitations
4.2 Transportation options to medical care for Central Washington residents
5.0 RECOMMENDATIONS
6.0 LITERATURE REFERENCES
1. INTRODUCTION
This survey study assessed the transportation needs of Central Washington state communities along the I-90/I-82 corridor for patients referred to specialized medical care in Seattle, Spokane, and other urban centers more than one hour away by car. This research was conducted throughout the fall and winter of 2023 to inform the Federal Railroad Administration (FRA) and Washington State Legislature and Washington State Department of Transportation (WSDOT) regarding possible benefits of restoring Amtrak North Coast Hiawatha (NCH) passenger rail service between Chicago and Seattle which, within central Washington, aligns with the I-90/I-82 corridor.
The NCH was Amtrak’s long-distance passenger train route serving Chicago, Minneapolis/St. Paul, southern Montana (Billings, Helena, Missoula), Spokane, & Seattle. The service was discontinued in 1979 due to lack of federal funding. Throughout most of its history, within Washington, the NCH operated between Spokane and Seattle on Burlington Northern Santa Fe tracks over Stampede Pass. Station stops within Washington were Spokane, Pasco, Yakima, Ellensburg, East Auburn, and Seattle.
Both quantitative and qualitative data were collected (see 5.1). This survey data may inform a benefit-cost analysis to determine the benefits and costs to society of establishing Washington state sponsored passenger rail service along the route. This survey was approved by the Pacific Northwest University of Health Sciences Internal Review Board.
2. BACKGROUND
According to Washington state law, RCW 81.66.010, people with special transportation needs are “those people, including their attendants, who because of physical or mental disability, income status or age, are unable to transport themselves or purchase transportation.” As of 2019, almost half of the Puget Sound (greater Seattle) region’s population (47%) had specialized transportation needs, whether they were an older adult (aged 65 or older), youth (age 5-17), a person with low income (household income under 200% of the federal poverty level), or a person with disabilities[10]. These groups tend to rely more heavily than others on public transit and specialized transportation to meet their daily needs. Comparable data from Central Washington is unavailable, but likely similar in scope, and urgently needed to plan transportation.
The U. S. Department of Transportation (USDOT) requires a Benefit-Cost Analysis (BCA) to support funding decisions for infrastructure investments, such as establishing passenger rail service, where an applicant is seeking discretionary Federal support[1]. A BCA is a systematic process for identifying, quantifying, and comparing expected benefits and costs of a potential infrastructure project[1]. USDOT provides guidance material which describes an acceptable methodological framework for purposes of preparing BCAs for USDOT discretionary grant applications. USDOT encourages applicants to incorporate this methodology into relevant planning activities, regardless of whether the project sponsor seeks Federal funding[1].
Passenger rail in the US was displaced by private automobiles after the advent of the Interstate ‘freeway’ system; chosen in the 1950s by President Eisenhower over expanded rail as the preferred transport for US national security. Passenger rail withered as cheap gas, subsidized highways and stylish cars made travel fast, cheap, easy and fun.
Passenger flights from Seattle serve Yakima and the Tri-Cities area, but no direct flights connect either city to Spokane. Connecting flights through Seattle take 4-9 hours and as of late 2023 cost $600-$900. Air transport is too expensive for most patients, who are already economically and emotionally stressed by illness, insurance uncertainties, lost work and family care time, and other constraints. Additionally, there is no current passenger rail service in Yakima or Kittitas Counties.
A Seattle to Spokane twice-daily Washington state sponsored passenger rail service via Stampede pass is technically feasible, has a high level of community support, and could generate significant ridership, especially within the Kittitas and Yakima Valleys[2].
The Passenger Rail Investment and Improvement Act of 2008 (PRIIA) requires that the operating and capital costs of routes of 750 miles or less be provided by respective States. This is referred to as “state sponsored” service.
Benefits of passenger rail service to central Washington include reduced greenhouse gas emissions[4], reduced vehicle-miles-traveled[4] by modal diversion6 and improved safety benefits (from reduced highway fatalities, property damage, and injuries)[5]. However, the health benefits of improved rail access to specialty health care providers are unknown.
USDOT recognizes that there is value to society from “Health Benefits,” and “Agglomeration Economies,” i.e., benefits gained by more efficient use of common resources and facilities such as hospitals and schools[1].
To our knowledge, there has been no prior survey of Washington state medical providers or medical service users (‘patients’) regarding rail access to specialty medical care in large cities by patients in rural or tribal areas.
2.1. Primary outcome measures
- The number/types of patients/conditions who travel more than 1 hour by car for specialty medical care.
- The modes of travel used to access specialty care unavailable near their home.
2.2. Secondary outcome measure(s)
- Provider demographics and personal experience with passenger rail
- Provider perception of safety & utility of rail transport to medical specialty care.
2.3. Hypothesis
Restoration of Amtrak NCH passenger rail service and establishment of Washington state sponsored service between Seattle and Spokane on existing Burlington Northen Santa Fe tracks over Stampede Pass will improve access for residents of Central Washington communities to specialized medical care in Seattle and Spokane.
3. RESULTS
Responses were gathered through a variety of healthcare professional organizations throughout the I-90/I-82 corridor, including the Washington State Medical Association (WSMA) and associated county medical societies, Washington Academy of Family Physicians (WAFP), Yakima Valley Farm Workers Clinic, MultiCare Yakima Memorial Hospital, Kittitas Valley Healthcare, and the Yakama Indian Health Service Unit. 18 responses in total were submitted by a respondent pool consisting of physicians, physician assistants, and nurse practitioners. This represents a 1.1% response rate of the total combined pool of nurse practitioners (314), physicians (1077), and physician assistants (237) in Chelan, Yakima, and Kittitas Counties as of 2021[3,7,8].
3.1. Specialty Care Cities (445 patients total monthly)**
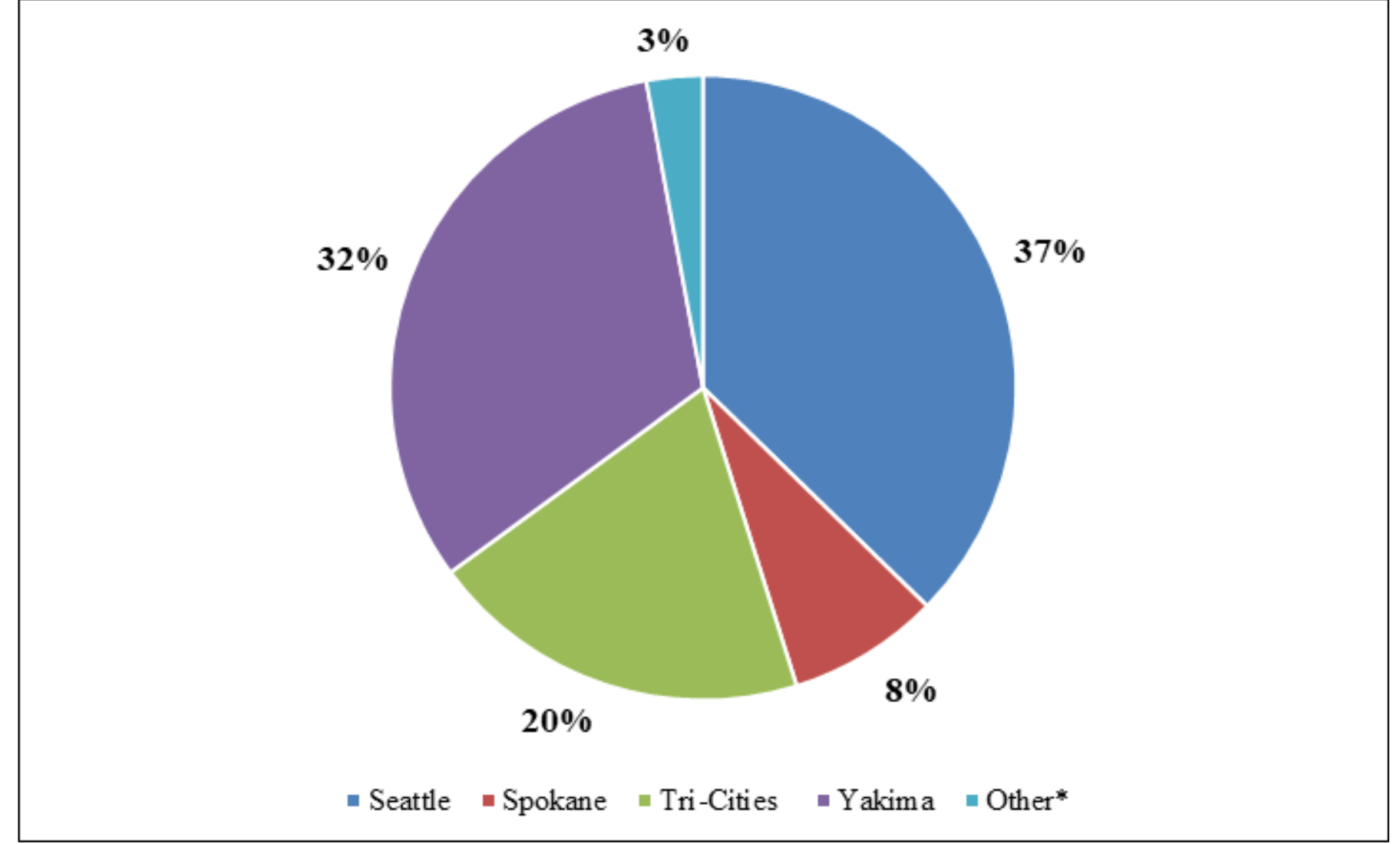
**Respondents were asked how many patients they referred monthly to the cities listed.
*Other cities include Portland, Bellevue, Issaquah, and Wenatchee.
3.2. Respondents’ practice locations along I-90/I-82 corridor*
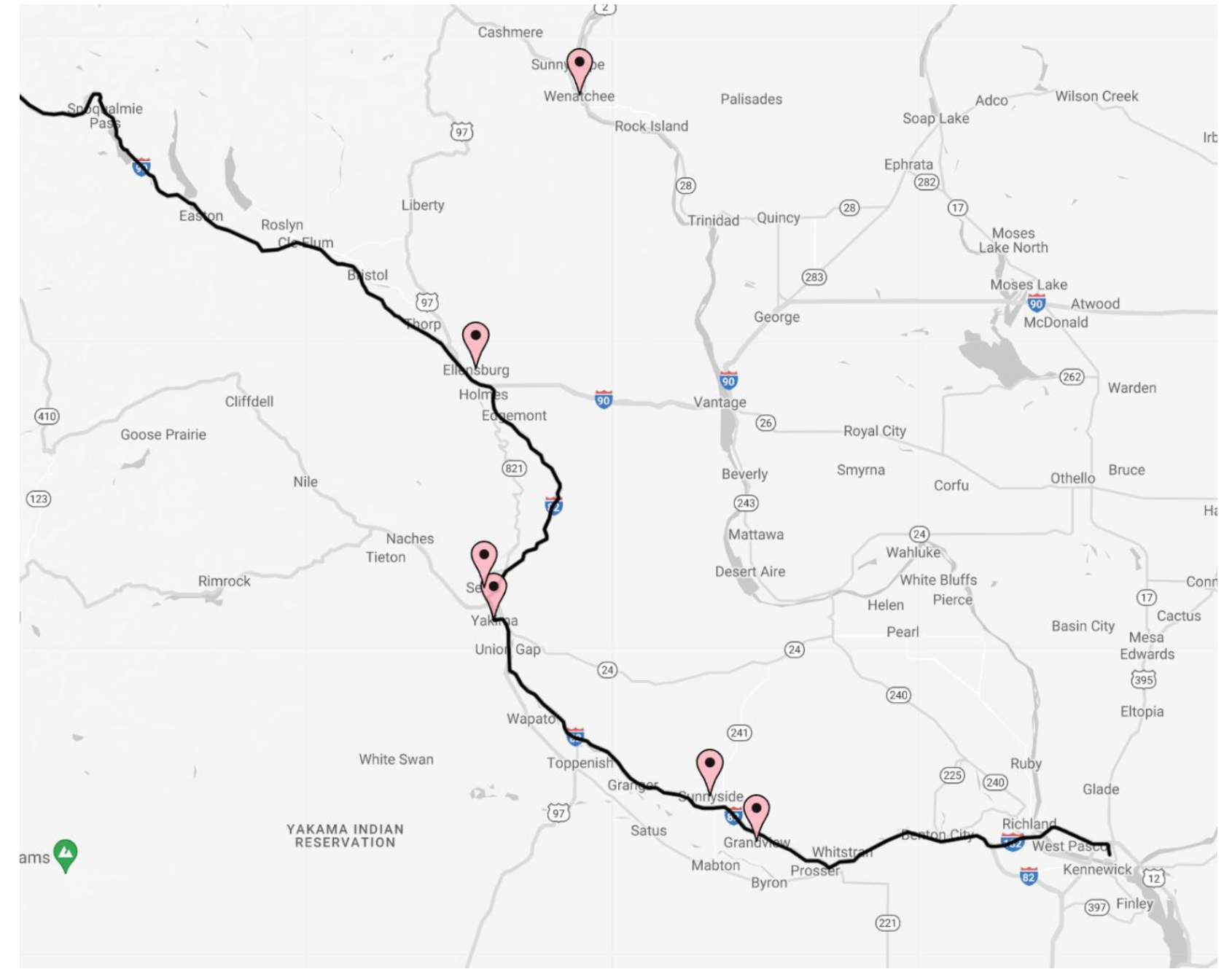
*The I-90/I-82 corridor between Seattle and Pasco as pictured above aligns with the former rail route of the North Coast Hiawatha.
Respondents: Wenatchee – 2, Ellensburg – 3, Selah – 1, Yakima - 10, Sunnyside – 1, and Grandview – 1. Map was created via Map Maker.
3.3. Primary mode of transportation to specialty appointments.
| Responses (17 total) | |
| Patients drive themselves by car or are driven | 88% (15/17) |
| Paratransit/medical transport services* | 12% (2/17) |
| Passenger bus services | 0 |
| Ambulance | 0 |
*People for People, Dial-A-Ride, clinic/hospital specific vans, etc.
3.4. Minimum train service required to benefit non-urgent patient transportation.
| Responses (18 total) | Responses (18 total) |
| None; trains would not help my patients to access specialty medical care. | 11% (2/18) |
| Daily trains are not needed; a few times a week would be enough | 11% (2/18) |
| Daily trains departing late evening, with overnight stay required, are OK | 6% (1/18) |
| Daily trains departing early morning and returning late evening (same day) | 72% (13/18) |
| Overall support for train service in some capacity to benefit patient transportation | 89% (16/18) |
3.5. Respondent prior experiences with passenger rail
| (Select all that apply) | Responses |
| Yes, light rail | 17% (3/18) |
| Yes, commuter rail | 11% (2/18) |
| Yes, passenger rail | 0% (0/18) |
| No, none were available, convenient, or safe to get me where I needed to go | 56% (10/18) |
| No, I either drove, rode carpools/taxis/ride-share, took buses, or walked/biked | 28% (5/18) |
3.6. Extended Responses
Participants were asked to briefly explain the type and number of cases in which patients faced transportation-related barriers to referred appointments. Extended responses were submitted by 15 of the 18 respondents.
“The largest problem for access from my area is pediatrics. I work in rural community health in Grandview Washington. Our patients do not have the means to purchase gas or sometimes even have a car to make it to their appointments for their children. Also, gynecological oncology has been very difficult to get my patients to, especially the 50–60-year-olds who don't know how to or have no means to access telehealth.”
“I would refer more patients for electroconvulsive therapy or ketamine but driving over the mountains during the winter is a significant barrier. Not all my patients have reliable transportation or someone to drive them to/from procedures.”
“There are limited specialties in Yakima particularly GI, infectious disease, pulmonology, rheumatology, vascular surgery, dermatology, endocrinology that the practices in town either so not exist or so not have capacity. Many of my patients are uninsured or agricultural workers who do not have their own transportation. I often have to make do with an electronic consultation or very long wait times for a local place. It's not just cost for patients but also time off work, childcare, or frailty/pain that prevents long car rides. Traveling over the pass in bad weather also prevents access to care.”
“Many patients are unable or unwilling to travel to Seattle or Tri-Cities during the winter months due to concerns about road conditions.”
“There are significant access problems for my patients who cannot drive themselves to appointments."
“Probably 20 patients. Missed or rescheduled appointments delaying care including referrals for potential malignancy and for high-risk prenatal care. Sometimes they don't miss an appointment but have huge stress getting there especially if bad weather.”
“In the winter months, patients are often not able to get across Snoqualmie pass to Seattle for specialist appointments and surgery. I have also had 3 to 4 patients who were not able to secure transportation to specialist appointments in Seattle due to personal finances or having no available car or driver.”
“Inability to drive because of age or physical disability with working relatives that could not free themselves up from work to drive.”
“Multiple people who need skilled spine surgery to avoid potential permanent disability are unable to afford transport to Seattle and later end up in the ED and are airlifted to emergent surgery. This drives up healthcare costs and provides worse outcomes and higher morbidity for the patients. This has happened about 10 times in the last 1.5 years. “
“Loss of an Eye due to pass closure during winter. Worsening neurological status after bleeding
because of time of travel. “
“Patient not able to drive in winter to Seattle for consultation with hematologist and spine surgeon. Care delayed 4 months causing prolonged suffering.”
“Mainly insurance but transportation a close second”
“Barrier has generally been weather, and this is unreliable in the winter months.”
“I have many patients who are unable to get to Seattle for the specialty care they need. Some specialty services are limited here in Yakima and patients wait for longer than I would like for them to be seen because they are unable to travel. This is most notable during the winter months (Nov-April) when getting through the pass can be difficult.”
“1. patients often fearful of driving in the Settle metropolitan area (Seattle/Bellevue/Issaquah) 2.Don't feel safe driving over mountain passes in inclement weather (Seattle metro area AND to Yakima)”
4. ANALYSIS & DISCUSSION
4.1. Transportation options to medical care for Central Washington residents
Transportation to ‘hometown’ medical care is beyond the scope of this survey, which is limited to the question of access to specialty care beyond a 1-hour drive. We also did not address the medical care ‘desert’ of obstetric care in small towns. Despite post-COVID expansion of telehealth care, physical office visits are often still required; especially for specialty care that is unavailable in smaller towns and cities. 6.2% of Washingtonians over the age of 16 do not have a driver’slicense, and 5.2% do not have a car[9]. They still need transportation to medical care.
Most patients who require specialty care go to Seattle, Yakima, or Tri-Cities; all along the I-82, I-90 and Hiawatha route. Survey results confirm anecdotal reports that access to care is limited by lack of public transportation to those cities. Most of those who must travel—88%—do so by private auto, often the only mode available. We did not survey medical providers about the travel mode preference of their patients—this question must be asked of respondents in a future BCA.
Driving can be convenient for those with cars or drivers. However, travel to Seattle by car over Snoqualmie Pass during winter is treacherous and often impossible due to frequent highway closure by snow accumulations and resulting collisions and has resulted in prolonged suffering and delay of care. This is a recurrent theme amongst respondents’ transportation-related barriers to care (see 3.6). While passenger rail can be less limited by snow, collisions, and road closures, service can still be disrupted by inclement weather. There are numerous examples of the Amtrak Cascades service in Washington state having been delayed (and passengers transported by buses) due to mudslides on the tracks to the extent that WSDOT has received Federal grants for mudslide mitigation along the Cascades route. Inclement weather also impacts on-time performance of the Amtrak Empire Builder service from Chicago to Seattle as it crosses the Rocky Mountains during winter months.
The cost associated with owning a vehicle, physical disability preventing patients from driving, and poor access to drivers for patients unable to drive themselves were also cited as significant barriers to care and, in some cases, led to greater healthcare-related costs (see 3.6).
Most (72%) providers indicated that the minimum train service required to benefit non-urgent patient transportation would be services with daily trains departing early morning and returning late evening (see 3.4). Even though most physicians are trained in large urban centers, most (56%) had no prior personal experience with passenger trains; as it was described as not available, convenient, or safe. This is consistent with the dearth of passenger rail transport in the US for the past two generations.
Finally, the spontaneous narratives provided information that cannot be assessed with brief survey questions; confirming the poignant stories of travel needs identified by WA State law: “specialized transportation needs, whether they were an older adult (aged 65 or older), youth (age 5-17), a person with low income (household income under 200% of the federal poverty level), or a person with disabilities”. Sick children, women with cancer, poor people who cannot afford a car or gas, those with chronic conditions that worsened due to delayed access—all are affected by transport barriers to medical care.
4.2. Study Limitations
We decided to survey medical provider perception as a proxy measure of medical service user needs, from easily available Washington State Medical Association and other membership email lists. The study is limited by a low response rate, despite support by Washington State Medical Association to encourage member participation. Medical care providers are busy, especially prior to winter holidays; with limited time. Also, many do not consider transportation to health care as a medical practice issue, which is why we queried their own rail experiences. Finally, because passenger rail has not been available for 42 years in the area, it is not considered as a current option to access medical care or general transport.
5. RECOMMENDATIONS
We recommend that FRA, Amtrak, WSDOT and WA State Legislature conduct formal BCA of restoration of the North Coast Hiawatha; for general rail service between Seattle and Tri-Cities WA, and specifically for patients who require transportation to specialty medical care in Seattle and Spokane. This pilot study demonstrates the transport barriers to care; causing significant care delays and increased total cost to the medical system of providers and insurers. The BCA must specifically assess medical care transport needs by surveying users (patients). Disability Rights Washington (https://www.disabilityrightswa.org/) is an essential resource, as well as patient advocacy groups, local health care groups, and insurers in Central Washington.
The BCA will require support and funding by the WA State Legislature. All Aboard Washington (www.aawa.us) will ask the legislature to provide funding for a benefit-cost analysis of east-west passenger rail service via Stampede Pass. The survey results will support such as request, for medical reasons.
6. LITERATURE REFERENCES
- U.S. Department of Transportation. Benefit-Cost Analysis Guidance for Discretionary Grant Programs. 2022 Mar.
- Sproul I. Feasibility of an East-West Intercity Passenger Rail System for Washington State. 2020 Jul.
- Yen W. 2020-21 Physician Supply Estimates for Counties: Washington State. 2021 October.
- Stacy C. Davis; Robert G. Boundy. Transportation energy data book. Oak Ridge, TN: Oak Ridge National Laboratory; 2021.
- Hu, Patricia; Schmitt, Rolf R.; Robinson, Ramond; Nguyen, Long; Moore, William H.; Baunee, Aaron; Culotta, Kalle; Hocevar, Hannah; Kimmel, Sari; Stacey, Mikki; Wingfield, Alpha. Transportation Statistics Annual Report 2022. United States Department of Transportation; 2022.
- Washington State Department of Transportation. Ultra-High-Speed Ground Transportation Business Case Analysis Final Report. 2019 July.
- Yen W. 2020-21 Physician Assistant Supply: Estimates for Washington. 2022 May.
- Yen W. 2017-21 Advanced Registered Nurse Practitioner Supply in Provider Networks: Estimates for Washington. 2022 November.
- Washington State Legislature Joint Transportation Committee. NONDRIVERS: POPULATION, DEMOGRAPHICS & ANALYSIS. 2023 Jan.
- Puget Sound Regional Transportation Plan, 2022
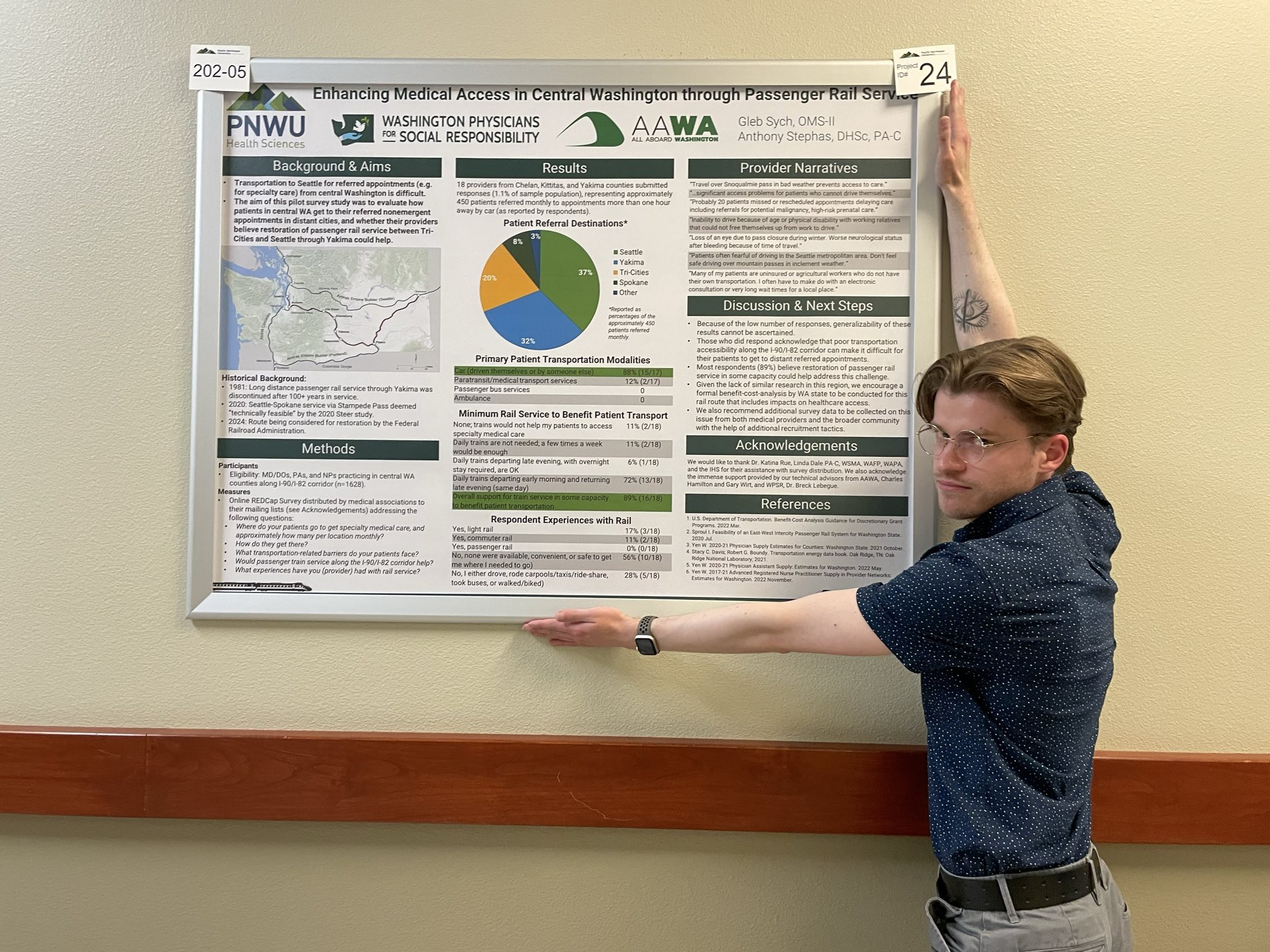
Gleb Sych, AAWA board member and student co-investigator of the the recent Medical Provider Survey on the Impact of Restoring Passenger Rail Service in Central Washington https://arr.as/g reports: “I presented the poster at my school's symposium last week and it went well! Many folks were curious about the subject and were excited to hear about the prospect of passenger rail potentially returning to Yakima. Many also asked if we plan to follow up with another round of data collection.”